
Overview of FCA
Functional Cognitive Activities (FCA) is a comprehensive system for addressing functional cognition in persons with cognitive deficits due to acquired brain injury: stroke, traumatic brain injury, tumors, etc.. OT, PT, ST and activities therapists can use the structured system to plan treatment sessions that incorporate the skilled use of therapeutic tasks and activities to foster independence.
The 8 Levels
The therapist chooses functional therapy tasks and activities based on 8 sequential levels of functional cognitive performance:
Level 8: “Planning/Multi-Tasking”
Level 7: “Out the Door”
Level 6: “Organize the Therapy Hour”
Level 5: “Beyond the Room”
Level 4: “Follow a Time Schedule”
Level 3: “Moving Around the Room”
Level 2: “What Time is It?”
Level 1: “Initiating the Next Step”
How to Determine a
Starting Level
The therapist uses the FCA Evaluation Scale plus other cognitive screens, tests and scales to determine the starting functioning level.
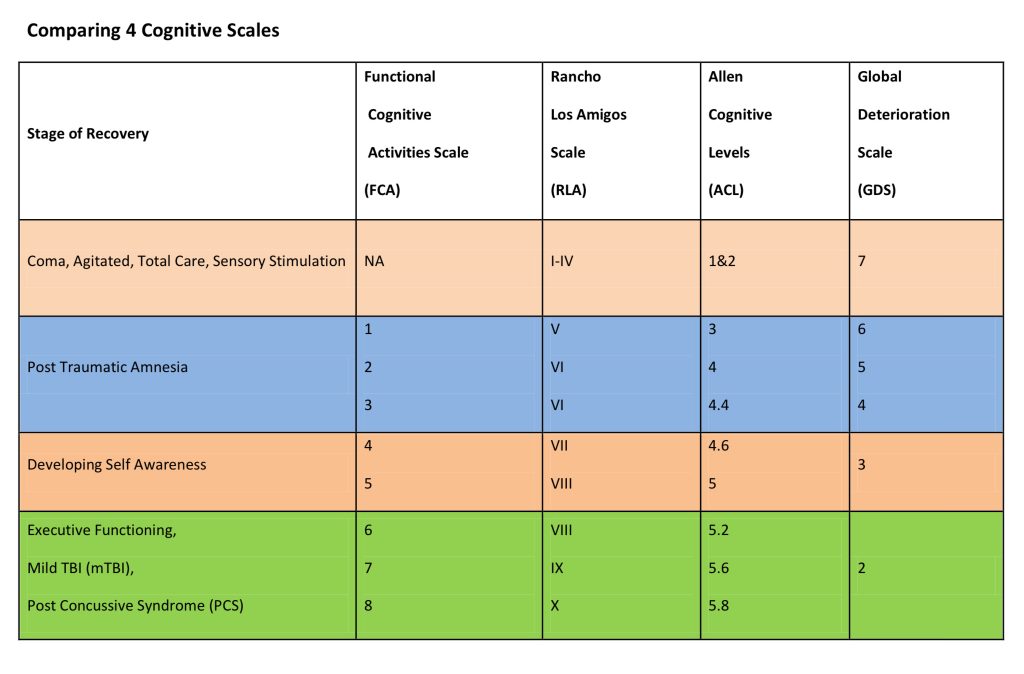
The chart below compares the 8 Functional Cognitive levels to equivalent levels in other scales:
FCA Website
Once the therapist determines the appropriate level – he uses the website to choose and print specific tasks and activities to use in a session. Activities begin with having the person practice initiating the next step in a sequence of basic ADL tasks; gradually progressing to the highest cognitive level which involves planning and multitasking to carry out complex ADL. The website also includes access to an evaluation scale, a progress guide for establishing and measuring progress toward goals.
$25.00 (online access)
The 3 Global Elements
A core concept of this approach is that the person’s cognitive performance level is based on 3 global elements of cognitive functioning rather than scores on cognitive sub-skills. It is the awareness and management of these 3 global elements that indicate how independent a person will be.
Interpersonal relationships: self awareness, social skills, comprehension, self regulation
Environment: physical space, personal awareness, body scheme, safety awareness, community, buildings
Time parameters: orientation, time limits, schedules, estimating time, multi-tasking, project deadlines
The 8 Cognitive Functioning Levels in Detail
Level 1: “Initiating the Next Step” is the lowest level of functioning addressed in this therapy system. The person typically sits until told what to do. He is not oriented to time, environment or others. He does not initiate conversation and has trouble following basic verbal directions. The goal is to get the person to initiate to moving on to the next step in a sequence. This can be as simple as carrying through all the steps in the basic task of brushing teeth. Hopefully the person will be slightly higher functioning and will learn to initiate moving on to the next task in series of tasks such as brushing teeth, combing hair, putting on deodorant, etc. This level requires intensive training and repetition.
Level 2: “What Time is It?” emphasizes having the person attend to time throughout therapy sessions so that he will begin to initiate moving on to the next task or exercises based on what time it is. He is starting to follow more complex verbal commands and respond appropriately to others. He is beginning to find things that are not in his immediate field of view. There are 2 types of activities that can be practiced in therapy sessions: “Time Blocks” and “Interrupts”. The time changes need to be in short time intervals (5,10, or 15 minutes) so the person gets repeated opportunities to practice. At this level the person frequently loses track of time if too much time elapses between tasks.
Level 3: “Moving Around the Room” is the last of the low levels of functioning. The person is emerging from the post-traumatic phase of recovery as he is retaining new memories and becoming oriented to the time and his environment. The goal for therapy at this level is to have the person navigate his way around the room to carry out a variety of tasks. He may now be doing some simple reading so tasks can be more complex. He also is now oriented to the time of day so is able to initiate moving on to the next task at the specified time, although he may need an alarm to compensate. He needs to have his errors corrected for him so that he does not learn inappropriate ways to carry out tasks.
Level 4: “Follow a Time Schedule” is the beginning of mid-level functioning. Since the person showed at earlier levels that he knows what time it is, he is now expected to not only keep track of what tasks to carry out during the session – but also remember to start and stop them on time. At this stage the person has learned to find his way within the immediate therapy room and is branching out to nearby roooms. He may be using a compensatory device (low tech or high tech) to compensate for deficits in time management or memory. He may need supervision to carry out unfamiliar tasks. He often does not realize that he is making errors until they are pointed out to him.
Level 5: “Beyond the Room” is the level where the person starts to practice finding his way within buildings. There are 3 types of activities to practice: “Repeats”, “Sequenced Routes” and “Complex Scavenger Hunts”. A main focus at this level is to determine what navigation method works best for the person to find his way. This includes using maps, reading signs, attending to landmarks, asking for directions and reading directions. At this level the person can attend to time points while engaged in complex tasks. He is also starting to use mental strategies to keep himself organized and stay on time. He is starting to become aware that he is having difficulties but may deny it.
Level 6: “Organize the Therapy Hour” is the first level where the therapist begins to reduce the amount of structure he provides the person during the session. Thus the activities at this level are designed to have the person practice executive functioning skills. The therapist still declares what tasks and/or exercises he wants the person to complete – but it is up to the person to organize those tasks and exercises. He needs to plan by prioritizing tasks according to rules, adhering to time limits, estimating time needed for tasks and finally carrying them out. A major emphasis at these higher levels is to guide the person in “thinking about what he is thinking about” to develop self-awareness.
Level 7: “Out the Door” is the community reintegration phase of cognitive rehab. The activities at this level allow the person to show that he is safe and efficient navigating unfamiliar community environments. Persons who are at this level are on the way to being independent – able to care for themselves and manage in the community including driving or using public transportation. Lesson plans for this level have the person practice planning efficient routes and attending to safety in community settings. He may need to use compensatory devices or mental strategies to make up for his deficits. He is beginning to develop insight into his problem areas and learning to compensate as necessary.
Level 8: “Planning/Multi-tasking” is the highest in the hierarchy. Persons at this cognitive level have good potential to return to their pre-morbid roles including home management, return to school and work. The therapist asks the person to carry out complex projects and high level multitasking activities during the session. There is very little structure provided to the person as he is presented these activities. The therapist’s role is to provide guidance to the person and get him to think about how he can be more efficient as he performs higher level compensatory techniques to carryout out projects. The person is taught to question what he is doing and generate alternative solutions when problems arise.
back to top
The 3 Global Elements in Detail
Interpersonal Relationships and Self Awareness
This is arguably the most important of the 3 global elements. If the person is going to be independent to any degree – he must be aware of that he has cognitive deficits. Otherwise he will have to be supervised to some degree in daily life. The highest level of self awareness is developing insight into the reason for the deficits which indicates total understanding of his situation. Before the person develops self awareness he must be able to communication effectively with others, follow instructions, control his emotions and monitor his behavior.
Subcomponents of interpersonal relationships and self awareness include:
initiating communication, orientation to others, phone use, expressing emotion, following commands, reading comprehension, self regulation, error detection and correction, engaging others, setting goals.
Time Awareness and Management
Being able to monitor time during daily activities is very important to living independently. At the beginning stages of time management the person must simply be able to initiate switching from task to task. After that he progresses to showing that he can interrupt what he is doing at a particular time of day to change tasks. This leads to using a time schedule to complete a series of tasks. Next the person moves on to creating his own time schedule for completing multiple tasks by considering time limits, following rules, prioritizing tasks and estimating the time needed to complete them. The highest levels of time management include formulating, then implementing a plan to complete complex projects by a deadline while demonstrating effective multi-tasking to increase efficiency in daily life.
Environmental Awareness and Management
Awareness of the environment begins with the person being aware of his own body image. It progresses to attending to objects within reach such as wheelchair brakes and walkers. Shortly after the person begins to scan the room around him for objects in his immediate field of view. As he starts to move around the room he is able to recall items that are stored in cabinets or closets. Next he attempts to organize items he needs for tasks as he works at a table or countertop so he can be more efficient. Soon he begins to find his way around the first floor of a building. He shows he can carry and keep track of where he keeps his phone, schedule or notetaking device. Once he demonstrates he can find his way in a multi-level building he ventures out into the community to carry out assignments. He can use maps or GPS when he is in unfamiliar areas.
back to top
Additional Cognitive Assessments
Commonly Used Cognitive Evaluation Scales
Cognitive scales are helpful to provide guidance on what functional tasks and activities are appropriate to use for the person at a specific level. Although scales are not standardized, they frequently identify the functional goals that need to be addressed by all members of the interdisciplinary team. Common scales are:
Allen Cognitive Levels (ACL)
Rancho Los Amigos Scale (RLA)
Global Deterioration Scale (GDS)
FCA Evaluation Scale*
Functional Cognitive Activities Evaluation Scale
This scale is used to determine the persons current performance regarding awareness and management of the 3 global elements of time, interpersonal relationships and environment.
Screening Tools
When therapy time or limited visits is a problem, screening tools can be done quickly to get a general idea of the person’s current cognitive status. Common screening tools in include:
Brief Interview for Mental Status (BIMS)
Mini-Cog
Montreal Cognitive Assessment (MoCA)
Mini-Mental Status Exam (MMSE)
St. Louis University Mental Status Exam (SLUMS)
Brief Cognitive Assessment Tool (BCAT)
Performance Based Testing
These tests involve having the person carry out a specific battery of real-life tasks. They require more including set up other than providing paper and pencil. Examples include:
Kohlman Evaluation of Living Skills) KELS
Executive Function Performance Test (EFPT)
Multiple Errands Test (MET)
Woodrow Wilson Executive Route Finding Test (ERFT)
Cognitive Performance Test (CPT)
Assessment of Motor and Processing Skills (AMPS)
Safe at Home Screening
Standardized Neuropsychological Evaluations
These evaluations test and analyze specific cognitive performance deficits such as memory and attention although they can be combined into one test battery. They take more time than all the other tools and are often more expensive. The tests are most frequently administered by speech therapists and psychologists. They are vital for research however the ecological validity of the results is frequently questioned. There are MANY to choose from but here are a few examples:
Stroop Test
Clock Drawing Test
Trail Making Tests
Test of Everyday Attention (TEA)
Rivermead Behavioral Memory Tests (RBMT)
Behavioral Assessment of Dysexecutive Syndrome (BADS)
… many, many, many more
Self Awareness Assessments
These assessments help the therapist, person and family members to examine the person’s current level of understanding and insight into his cognitive deficits. Self awareness is critical in fostering independence. Examples include:
Self Awareness of Deficits Interview (SADI)
Patient Competency Rating Scale (PCRS)
Awareness Questionnaire (AQ)
Dysexecutive Function Questionnaire (DEX)
Stroke Impact Scale (SIS)